

Something Abnormal lies Buried in England's Death Data

Early and ongoing analysis of Covid-19 mortality data demonstrates the following:
Mortality appears to go up after vaccination, usually within the first week or two.
The definition of being ‘vaccinated’ [wait 14 days after vaccination to be deemed vaccinated with 1 dose] avoids those mortality data being put in the Vaccinated total.
Similarly, by only being fully vaccinated 14 days after 2 doses, a whole chunk of data are removed potentially skewing any fair and unbiased comparison to the unvaccinated. Of course, the goal posts are moving again, with a 3rd; 4th; and X number of doses. Falsely adding the previously fully vaccinated to the unvaccinated column.
Just a cursory look at VAERS, with all its caveats, it’s not that difficult to see an early rise in mortality associated with vaccination, that in part explains the observations.
Fig. 1 VAERS Covid-19 and flu mortality after vaccination
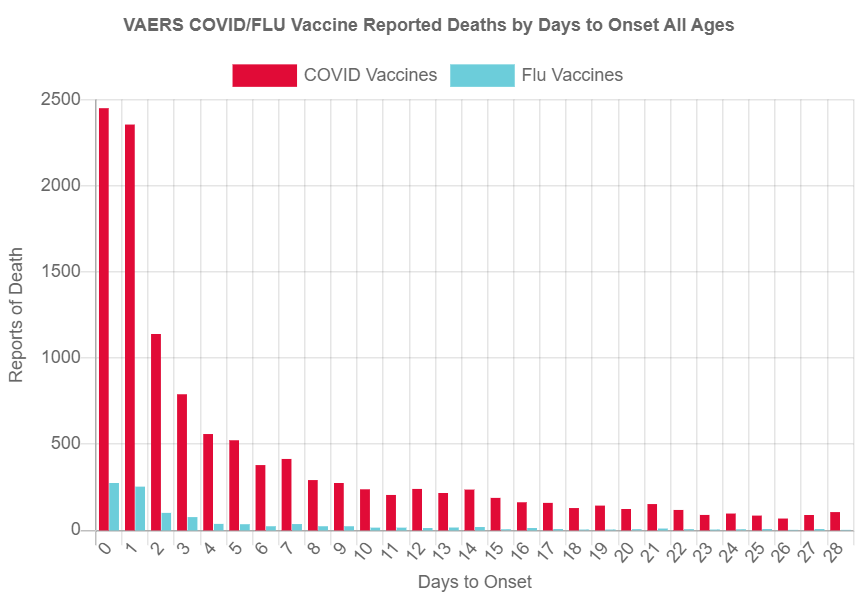
Source: OpenVaers
VAERS data demonstrate a significant rise in reported deaths associated with Covid-19 vaccines within two weeks post vaccination, with the main effect in the first 7 days. Comparison with influenza vaccines indicates orders of magnitude increase in reports.
For long term care facility (LTCF)residents, The CDC initially stated:
Reported deaths occurred 0–20 days after vaccination (median = 2 days)
And for non-LTCF deaths;
The median interval from vaccination to death was 3 days (range = 0–20 days).
Also, the initial Pfizer trial data demonstrated a transient suppression of the immune system lasting 3-5 days, which may help explain some the above observations.
Fig.2 Post vaccination changes in lymphocyte count over time

Source: Phase I/II study of COVID-19 RNA vaccine BNT162b1 in adults [Extended data]
Lymphocyte suppression in first week in vaccinated subjects. Note that the control sample was not suppressed.
And let us not forget all the other potential contributory factors:
The adage Sola dosis facit venenum or the dose makes the poison is a basic tenet in toxicology, and will be no different here with Covid vaccines. Apart from all the other serious effects that have already been demonstrated as a result of vaccination heavily implicating spike protein, repeatedly dosing human beings with Covid 19 vaccines, potentially inhibiting DNA repair and causing cellular senescence, with the attended risks of cancer and decreased life-span do not bear thinking about. In the case of the developing foetus, would that risk entail never having a life to span?
Source: Vaccine Induced Cellular Ageing
Vaccine-induced immune thrombotic thrombocytopenia (VITT); Heart damage; and more…
But what of recent events and how might they be linked to observations of the vaccinated mortality data being mis-categorised as unvaccinated?
Dr. Martin Neil from Queen Mary, University of London and colleagues published a paper entitled Latest statistics on England mortality data suggest systematic mis-categorisation of vaccine status and uncertain effectiveness of Covid-19 vaccination where they address this mis-categorisation of Covid-19 vaccinated and unvaccinated deaths: adding vaccine deaths into the unvaccinated column. They summarise the possible mis-categorisation processes.
Fig. 3 Possible mis-categorisation processes of Covid-19 vaccinated & unvaccinated deaths

From fig. 3 we see that (mis)reported deaths categorised as unvaccinated (less than 14 days after vaccination) (first blue arrow) should be categorised (actual categorisation) as first dose vaccinated; and death categorised as vaccinated first dose (third blue arrow) should be categorised as second dose.
The researchers state that the mis-categorisation and other anomalies in the data cast doubt over the conclusion that the vaccinated suffer less mortality than the unvaccinated:

We have explained that various social and ethnic factors are very unlikely to explain these odd differences in the ONS data set. Absent any other better explanation Occam’s razor would support our conclusions. In, any event the ONS data provide no reliable evidence that the vaccine reduces all-cause mortality.
One chart I’d like to highlight is shown in figure 4.
Fig. 4 Total deaths, total population change and total deaths unaccounted for by total population change for all age groups (weeks 1-37, 2021)

The brown lines shows the total deaths per week in the England; and the blue line shows the change in the population. As the population is standardised, the blue line should exactly reflect the deaths (brown) line. The difference between the two lines is depicted by the grey line.
But there’s a major problem with the government data: it does not track correctly in the first 12 weeks. Look at the peak in the deaths (brown) line at week 3. it indicates approx. 15,000 deaths but the population (blue) line has only decreased by 5,000. The grey line indicates the missing 10,000 deaths.
The chart continues mismatching until it makes a steep correction down to week 12, and then the two lines are in synch: population changes match deaths, indicated by the grey line staying at zero.
Dr Neil and his colleagues describe it, thus:
The total number of deaths unaccounted for by the change in total population is around 10,000 per week until week 10 and positive until week 12. This should not be possible. Likewise, logically we might expect the total population change to be negative across the whole period but remarkably it is positive between weeks 8 to 10, suggesting population has somehow been added to the data set. From week 12 the decline is predictable and steady as expected but in the first three weeks the decline is much steeper before the period in which population is added back in. After week 12 the total change in population exactly matches the total deaths, as expected. [My emphasis].
Importantly, they add:
This suggests something odd is going on up to week 11, when a possible systematic bias is introduced, which is then ‘recovered’ by week 12 and the bias disappears thereafter. We cannot explain why this pattern exists, but it is clearly a concern. [My emphasis].
Clearly a concern…. bias is introduced…..which is then ‘recovered’?
Are we witnessing bias and mis-categorisation that skews data and misleads the public to believe that Covid-19 vaccination is preventing mortality? And just how does bias, once entered into the data, miraculously recover itself?
Data cannot do that unaided…
But is there any way we can interrogate the data further?
Numbers can conform to patterns in nature with predictable frequencies, even death numbers. And if the data sets do not fit that pattern then we can ask legitimate questions as to what has altered them.
One such pattern is described in the law of anomalous numbers. That describes a specific expected frequency for each digit from 1 - 9 in the first position of a number. For example, the number 1 will appear 30.1% of the time in the first position of a number eg 1754; and the number 9 will appear 4.6% of the time in the first position eg 9754. There are also expected frequencies for the first 2 digits of any number…and so on. It seems quite unbelievable but the law of anomalous numbers is so established and reproducible that it is used in Court to prosecute accounting and election fraud.
A common name for the law of anomalous numbers is Benford’s Law.
We can use Benford’s Law to look at unvaccinated data, as that should conform to Benford’s distribution. As the vaccinated data has had a vaccine intervention, it should not conform to Benford’s Law. Analyses on both Covid-19 mortality & All-cause mortality data for the unvaccinated from England’s ONS is below.
One digit analysis for the unvaccinated Covid-19 mortality stayed within 95% confidence intervals.
Fig. 5 Benford’s 1 digit analysis of unvaccinated Covid-19 mortality data

Benford’s 1 digit analysis does not demonstrate a breach of confidence interval and comports with Benford’s Law.
Fig. 6 Benford’s 2 digit analysis of unvaccinated Covid-19 mortality data

Benford’s 2 digit analysis of Covid-19 mortality demonstrates breaches of confidence interval and does not fit Benford’s natural distribution. That raises a suspicion of corrupted data.
In addition, analysis of All-cause mortality data also demonstrated breaches of confidence intervals for both one and two digit analyses.
There are of course caveats: small data sets with lack of statistical significance. But whether standard statistical significance testing is appropriately sensitive to small number changes in that type of data set is debatable, even with larger data sets.
But what is interesting is the area of concern flagged-up by Dr. Martin Neil and his colleagues is also identified using Benford’s analysis of Covid-19 mortality & All-cause mortality data.
Fig. 7 Benford’s analysis of Covid-19 mortality & ALL-cause mortality data correspond with abnormal data pattern discovered by Dr Neil et al.

Both 1 and 2 digit analysis of ONS mortality data using Benford’s Law identified irregularities, some of which (indicated by black boxes) corresponded with an irregular data pattern previously identified by Dr. Neil et al.
I certainly do not suggest that the above is conclusive proof of wrong doing and have pointed out the caveats but it is more than apparent in the arena of Covid-19 that things just aren’t adding up when it comes to the number of deaths and cases.
Listen to Prof. Norman Fenton (co-author with Dr. Neil) who was interviewed and explains the findings from the Latest statistics on England mortality data suggest systematic mis-categorisation of vaccine status and uncertain effectiveness of Covid-19 vaccination paper and draw your own conclusion.
VIDEO LINK
